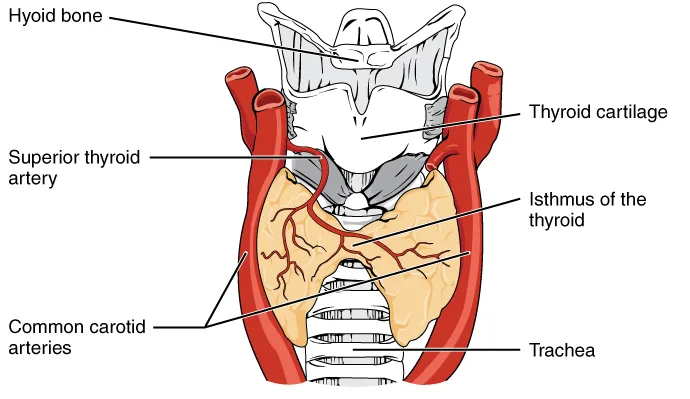

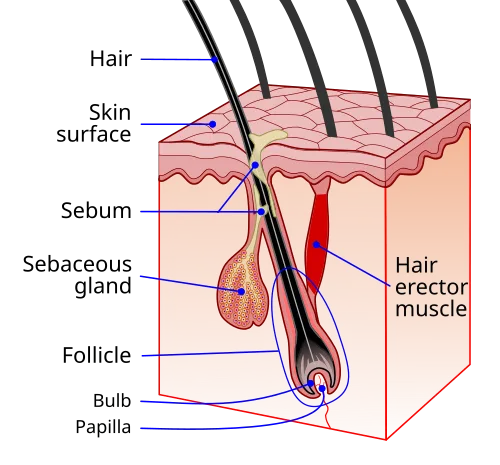
Thyroid hormone has direct effects on hair follicle biology. Thyroid hormone receptors are expressed on dermal papilla cells, and both excess and deficiency of thyroid hormone disrupt follicle cycling. Hypothyroidism produces classic telogen effluvium with prolonged shedding, often accompanied by dry, coarse hair texture. Hyperthyroidism causes a more rapid-onset diffuse shedding, sometimes with hair that becomes fine and limp. Both can mimic or unmask other forms of hair loss.
Despite being a textbook screening item, thyroid testing is sometimes overlooked in initial hair loss workups. A reasonable minimum panel includes TSH, free T4, and free T3. Subclinical thyroid disease, where TSH is mildly abnormal but free hormone levels remain in range, can still cause hair manifestations and is worth identifying. Autoimmune thyroid disease (Hashimoto's, Graves') also has independent associations with alopecia areata, adding another layer of relevance.
Correcting thyroid dysfunction typically resolves the hair component within 3–6 months as follicles return to normal cycling. Patients sometimes report that hair shedding worsens temporarily after starting thyroid hormone replacement, this is usually a transient telogen synchronisation effect as follicles reset their cycles, not a sign that the treatment is making things worse. For any patient with unexplained diffuse shedding, especially with associated fatigue, weight changes, or cold/heat intolerance, thyroid workup is non-negotiable.


Discussion (3)
AnonymousDad
5 months ago
This matches my own experience. Two years in and the picture is more nuanced than the early hype suggested.
Sophie L.
5 months ago
Really useful breakdown. The mechanism part was the bit I'd been struggling to understand.
Daniel R.
5 months ago
The cost/benefit case here is much weaker than the marketing implies. Useful that someone said it clearly.
Join the discussion
Free account. Read, like, save, and comment on every article.