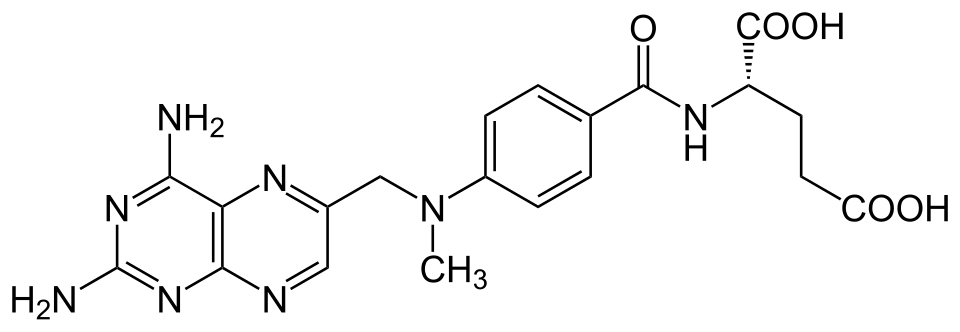

Methotrexate is a folate antagonist used widely in rheumatology, oncology, and dermatology. Its application in alopecia areata dates to the 2000s, with response rates of approximately 35–60% in case series and small trials when used for severe disease. The drug typically requires combination with low-dose corticosteroids in chronic alopecia areata protocols. In the era of JAK inhibitors, methotrexate has become less commonly used but retains specific value.
Typical alopecia areata dosing is 15–25 mg weekly oral methotrexate with folate supplementation. Combination protocols add low-dose prednisone (5–10 mg daily) for the initial months. Treatment duration is typically 6–12 months minimum before assessing meaningful response. Side effects include the standard methotrexate profile: GI symptoms, transaminitis, bone marrow effects, and teratogenicity requiring contraception in patients with reproductive potential. Regular blood monitoring is required throughout treatment.
Current use cases: patients who haven't responded to or can't access JAK inhibitors, those who prefer to avoid the JAK inhibitor side effect profile (particularly cardiovascular concerns), and combination strategies in chronic refractory disease. The substantially lower cost compared to JAK inhibitors makes methotrexate practical in healthcare contexts where the newer drugs aren't covered. Long-term safety data for methotrexate is extensive given its decades of use in rheumatology, this is well-known territory clinically, unlike the relatively newer JAK inhibitor class.


Discussion (1)
Priya S.
about 1 year ago
The point about effect size relative to existing treatments is exactly what's missing from most coverage of this.
Join the discussion
Free account. Read, like, save, and comment on every article.