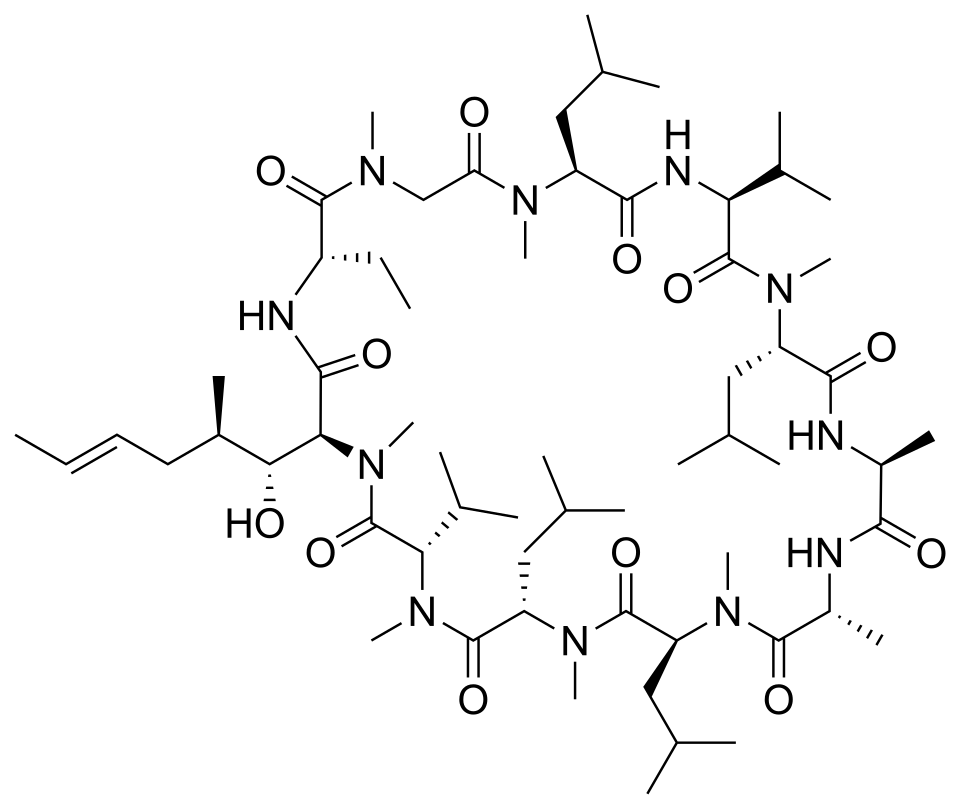

Cyclosporine has been used for severe alopecia areata since the 1990s, with response rates of approximately 45–65% in case series and small trials. Its mechanism, calcineurin inhibition blocking T-cell activation, directly addresses the autoimmune attack on hair follicles. The drug fell out of favour when JAK inhibitors emerged with better-characterised efficacy and somewhat different side effect profiles, but it remains relevant in specific clinical contexts.
Several modern use cases keep cyclosporine in the toolkit. Patients who haven't responded to JAK inhibitors sometimes respond to cyclosporine. Cost considerations matter, cyclosporine is dramatically less expensive than baricitinib or ritlecitinib, making it a practical option in healthcare systems without coverage for the newer drugs. Combination protocols (low-dose cyclosporine plus other immunomodulators) are being investigated as steroid-sparing strategies for chronic cases.
The side effect profile requires monitoring: hypertension (regular blood pressure checks), nephrotoxicity (creatinine and electrolyte monitoring), gingival hyperplasia, and hypertrichosis. Dosing for alopecia areata is typically lower than transplant-rejection prevention doses, which mitigates but doesn't eliminate these concerns. For patients without insurance coverage of JAK inhibitors and with significant alopecia areata burden, cyclosporine remains a defensible second-line systemic option with established efficacy data.


Discussion (2)
Daniel R.
8 months ago
The cost/benefit case here is much weaker than the marketing implies. Useful that someone said it clearly.
Karen W.
8 months ago
Anyone tried this in combination with low-dose oral minoxidil? Wondering if mechanisms stack.
Join the discussion
Free account. Read, like, save, and comment on every article.